 Augusta University
Augusta University
AUGUSTA, Ga. – Biofeedback therapy used at home is about 70 percent effective at helping patients learn how to coordinate and relax bowel muscles and relieve one of the most difficult-to-treat types of constipation, investigators report.
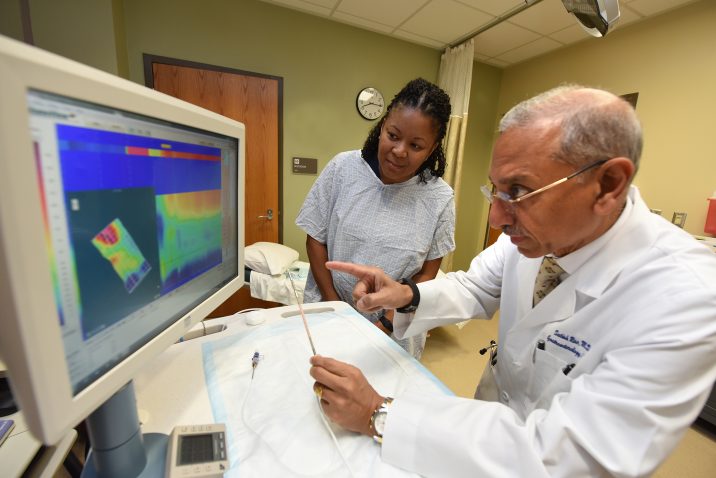
Standard treatments like more fiber in the diet, stool softeners, even laxatives, tend to be ineffective in patients with this type of constipation called dyssynergic defecation, says Dr. Satish S.C. Rao, director of neurogastroenterology/motility and the Digestive Health Clinical Research Center at the Medical College of Georgia at Augusta University.
About 15 percent of the U.S. population have chronic constipation, and about one-third of those individuals have dyssynergic defecation.
Familiar remedies don’t address these patients’ underlying issue of regaining the natural rhythm of contracting muscles at the top of the rectum to move stool out while relaxing muscles at the anal opening so stool can exit, says Rao, J. Harold Harrison MD Distinguished University Chair in Gastroenterology.
Rao led development of an office-based biofeedback therapy proven to help these patients better recognize the uncoordinated muscle movement and improve it. The American Gastroenterology Association, the American Neurogastroenterology and Motility Society and the European Society of Neurogastroenterology and Motility have all given the treatment a thumbs up.
However, limited training sites and the fact that many patients must travel long distances multiple times to get to those sites, had Rao and his team also wanting to make the effective approach more widely available and hopefully more cost effective.
The at-home system they developed appears to be equally effective, safe and less expensive, they report in the journal The Lancet.
“When healthy individuals attempt to poop, we increase the intra-abdominal and intra-rectal pressures and at the same time we relax the anal opening. We typically learn this when we are potty trained, then we never think about it anymore. Unfortunately, patients with dyssynergia don’t have that pattern. When these patients are attempting to stool, unbeknownst to them, they are pushing it back or just retaining it,” says Rao, the study’s corresponding author.
He notes some have had problems since childhood, others developed problems in adulthood from a variety of factors like back or hemorrhoid surgery, even pregnancy or hysterectomy.
“They started straining and gradually they changed their normal behavior to this abnormal behavior. The essence of biofeedback is built on converting patients with these patterns back to a natural, efficient pattern.”
The National Institutes of Health-funded study looked at a total of 100 patients, half randomly assigned to each group, from January 2005 to January 2010. Looking at all 50 patients who started in each arm, correction of the problem was seen in 72 percent of the home-based therapy group and 80 percent of the office-based group.
A total of 83 patients completed the study, 76 percent in the home-based group and 90 percent in the office-based group. Based on those who completed the study, at-home success rates were actually higher: 92 percent versus 84 percent, respectively.
Participants in both arms reported similar rates of improvement with key parameters like the number of complete, spontaneous bowel movements weekly, the investigators report. All participants also were better able to control their bowel movement, with both groups decreasing the time it took to expel a balloon — which gave them a surrogate sensation of pooping — and decreasing the number of times the balloons unexpectedly discharged.
“In every parameter we measured, the two approaches essentially matched head-to-head,” says Rao, other than costs.
Total costs, including travel time and transportation costs, were about twice as much for office-based therapy: $1,082 versus $1,942.
For the office-based therapy, patients had a training session with a nurse specialist followed by up to six, one-hour sessions over three months. A manometer helped determine whether they were contracting at the top of the foot-long rectum and simultaneously relaxing the bottom, or anus. Patients also learned a variety of breathing and other techniques to enable proper coordination. They received visual and verbal commands to improve coordination while seated on the commode.
Those selected for the home therapy arm also attended a single office training session to learn to use a reusable sensor probe connected to a handheld pressure monitor that let them know whether they were pushing appropriately in the two target regions. They were asked to sit on the commode twice daily and attempt 10-15 push maneuvers while looking at the pressure responses. Lights increased when the anus was being properly relaxed and decreased when they didn’t relax those muscles. A separate panel of lights would similarly respond to reflect the contraction of muscles at the top of the rectum.
At the start and conclusion of the training, participants were assessed with pressure monitoring at both key points in the rectum, a balloon expulsion test and a study of how rapidly waste, which is leftovers from digestion, passes through the colon using radiopaque markers. The six-foot long, continuously contracting colon moves waste from the small intestines to the rectum. “The colon is never inactive or still,” Rao says, but is a bit of a natural braking point in the gastrointestinal tract where fluids and other digestible residue get reabsorbed before we defecate. However when movement slows too much, as it does in about 60 percent of patients with dyssnergic defecation, it also contributes to constipation. While both study arms saw restoration of a more-healthy colon speed, the home-based group saw more significant improvement.
Both groups kept a stool diary over the course of the study and answered follow up questions about the tolerability and their acceptance of biofeedback therapy. While the home group said it was a little messy, they tolerated it well. Most study participants said they would recommend biofeedback.
The fact that both approaches produced similar results and home-based care is less expensive, should make it the preferred choice for these patients, the investigators write.
Now that they have the information, the investigators need a biotech firm to develop a home biofeedback system that can be widely distributed, Rao says. For the purposes of the study, Rao used a device made by a friend.
View a summary of the Lancet article here.



