Augusta University
Augusta University
During pregnancy, it is recommended that women visit their health care professional when they are eight to 12 weeks pregnant, then every four weeks until 28 weeks pregnant, then twice a month until week 36, then weekly until they deliver. Unfortunately, that isn’t achievable for many expecting mothers, with social determinants of health causing limitations to health care access.
Factors like financial status, transportation and education all play a role in mothers getting the care they need, but a main variable in this equation is the location in which they live.
A new two-part study out of the Department of Anesthesiology and Perioperative Medicine at the Medical College of Georgia at Augusta University suggests babies born to women who live in rural areas are at higher risk of complications at birth.
“We saw that patients who live in rural areas were prone to have lower Apgar scores, lower rates of prenatal care and higher rates of preterm delivery,” said Bibiana Avella, MD, a third-year anesthesiology resident at MCG who worked on the study.
An Apgar score, which stands for Appearance, Pulse, Grimace, Activity and Respiration, is an assessment that nurses or doctors conduct on newborns at one and five minutes after birth to assess their health. The score is based on those five criteria on a scale of 1 to 10, and scores less than six are considered “non-reassuring” and imply the baby might need more medical intervention.

For the study, the team of anesthesiologists analyzed the Apgar scores, as well as other variables like anesthesia type, maternal age, gestational age, race, BMI, education and employment status, comorbidities, substance use and the number of prenatal care visits of 2,953 mothers who delivered at Wellstar MCG Health from November 2018 to October 2023.

“We wanted to look at our data set and at the outcomes of the infants and see how it relates to their zip codes,” explained Mary Arthur, MD, anesthesiology residency program director and professor at MCG. “We also know that zip codes are closely tied to income levels in most of the counties in Georgia, so that led us to look at our patients along those lines.”
When people think about anesthesiologists, their first thought might not be about childbirth. However, anesthesiologists play an important role in obstetrics, managing pain and ensuring safety for the mother and baby by providing epidurals, spinal blocks and anesthesia for Cesarean sections.
Most of the profession’s tasks are based on caring for individual patients who come in, but Arthur challenged her residents to think outside the box when developing this study.
“I really wanted residents to start looking at patients from a different public health perspective,” she said. “Knowing that Wellstar MCG takes care of patients from most of the surrounding areas who come here for delivery. That’s basically what led to this study.”

Since 2010, nine rural hospitals in Georgia have closed, putting the state third in closures behind Texas and Tennessee. The problem is ongoing with more hospitals at risk for closures or reduced services due to changing demographics, physician recruitment challenges and increasing outmigration for labor and delivery services.
A map from the Georgia State Office of Rural Health shows 141 out of 159 counties in the state being medically underserved. This creates a domino effect for rural communities – health care professionals are forced to move to find work, businesses don’t have as many consumers and residents don’t have local access to specific health services.
In an effort to measure the impact of this on expectant mothers, the MCG team used the first part of the study to create color-coded maps for rural and non-rural areas the patients live in based on their zip codes. These maps, which serve as visual aids for each manipulated variable the team tested, highlight the disparities in maternal health care between rural and non-rural areas in Georgia and South Carolina.
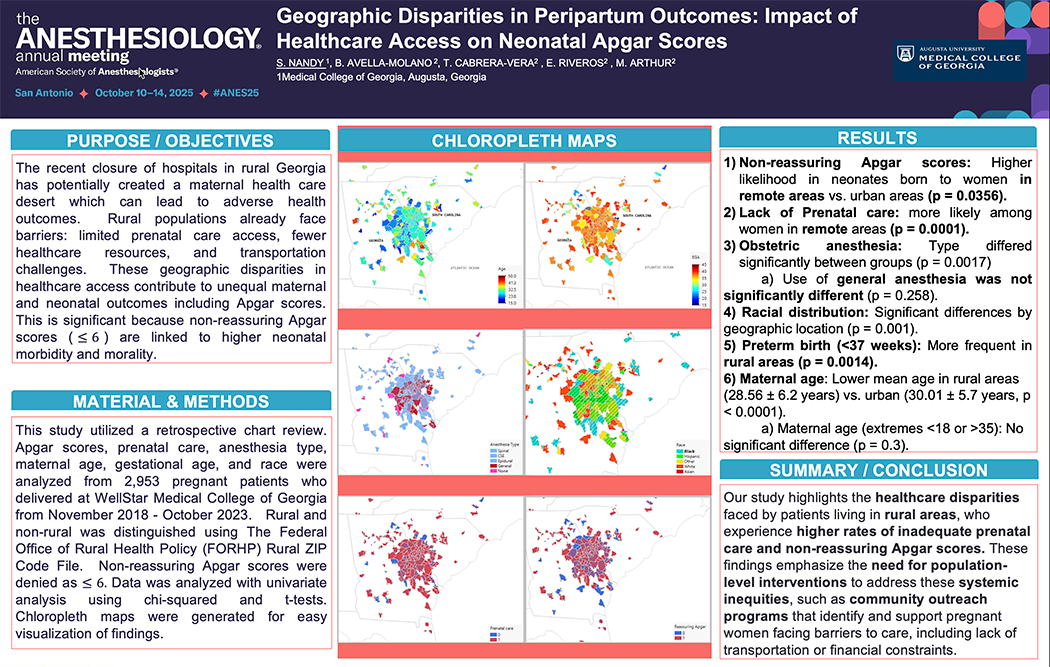
“The maps make it very easy to visualize those zip codes that link to poor neonatal outcomes,” Arthur said. “They’re also helpful for planning strategic interventions to help the people who live in those particular areas in terms of making sure there are outreach programs for mothers in those areas to have access to prenatal care.”
Of the 442 mothers from rural areas in the study, 108 (24%) had babies with non-reassuring Apgar scores, whereas 502 (20%) of the 2,510 mothers from urban areas had babies with non-reassuring Apgar scores. Based on the differences in sample sizes, this means that babies born to women from rural areas were about 30% more likely to have non-reassuring Apgar scores compared to babies born to women from urban areas.
Although it’s difficult to tell from this data set whether hospital closures are a root cause of lower Apgar scores, it’s clear that some variables affect pregnant women in rural areas disproportionately to those in urban areas.
In the second part of the study, the team found that 214 of the 2,953 women studied received no prenatal care and were 2.6 times more likely to have babies with non-reassuring Apgar scores than the remaining women who received prenatal care. They also found infants delivered vaginally and close to full-term births had better Apgar scores.
Based on these findings, the team deduced that these geographical disparities in health care access play a part in negative neonatal outcomes, including Apgar scores – and the lower the Apgar score, the higher the risk of morbidity or mortality for the infant.

“We used Apgar scores as our outcome variable, and then we saw which variables were affecting that outcome. We realized that BMI, gestational age, the number of pregnancies the patient had and other variables were influencing the Apgar scores for women in rural areas,” Avella said.
The study shines a light on the need for strategic interventions and outreach programs to serve these rural mothers and infants at a time when they need it most.
Arthur said the first step to solving the problem would be education.
“There are a lot of barriers for people who live quite a distance away from a main hospital, but education is one big thing. We need programs where we could actually reach out to these communities and make them aware of what they need to do during pregnancy,” she said. “We as anesthesiologists often don’t go into the field, but we work very closely with our obstetrics colleagues and other primary health care physicians in the same institution. This is not going to be one discipline’s effort; it has to be collaborative to impact the population we serve.”
Augusta University has outreach programs and resources in place, like the vidaRPM app and Maternal Care Model program, to help pregnant women and new mothers who live in rural areas. The program enrolls mothers who are in their second trimester all the way through six months postpartum, provides them with blood pressure monitors and scales and allows them to self-monitor their levels while receiving follow-up care from doctors and nurses.
MCG also has a Center for Digital Health, which focuses on providing telehealth services to patients near and far. It currently operates a tele-OB ED pilot program that provides rural hospitals with obstetrics instrumentation for identification and treatment of obstetric emergencies and a virtual way to connect mothers with physicians at Wellstar MCG Health.

“Telehealth is an amazing resource that MCG has,” Arthur said. “It’s amazing how people will be able to take ownership of their own health if they have the knowledge, and knowledge plays a very big role when it comes to something like this. A lot of people don’t know what they don’t know.”
Mobile clinics and transportation services, financial support initiatives and investment in obstetric infrastructure and workforce retention are also resources the team believes are necessary to improve neonatal outcomes in rural areas.
“When you start out with a small number of subjects in your data set, it’s sometimes difficult to make definitive conclusions for those numbers. So, next we’re going to increase our data set and see if what we’ve seen in this pilot study is actually real, and then that would inform us going forward on what we can do in the future. We’ve started talking to some clinics within Augusta that provide services to uninsured patients, and so, hopefully, once we get involved, our residents will be spending maybe one day a month there educating those patients,” Arthur explained.
The results of the study have also been a signal to the team that, as anesthesiologists, they need to be involved in the care of these rural patients earlier in order to ensure the best possible outcome for the mothers and their babies.
“We need to know about these patients earlier, that way we’re prepared in terms of getting maternal fetal medicine specialists involved, having our things ready in case we need to go for an emergency that’s not something in the scope of an obstetrician or gynecologist’s care,” Avella said.
The duo explained the results of the study provide ample evidence to support statewide policy efforts focused on maternal care access and highlight the need for future studies on how targeted interventions and outreach programs affect neonatal outcomes.
The team is currently working on publishing the manuscript for their research and plans to continue studying this population with a larger data set.
“Where a mother lives shouldn’t determine whether her baby starts life healthy,” Arthur said. “Yet, our research shows that rural mothers face real disadvantages, including limited prenatal care, which can increase the chance of complications at birth. The most important message is that prenatal care access matters, and non-reassuring Apgar scores are not random events – they reflect upstream inequities that are measurable, modifiable and addressable. Improving maternal health in rural and underserved areas requires coordinated clinical, community and policy-level action, and anesthesiology has a vital role to play in that effort.”